Lecture Details[]
Julia Choate; Week 10 MED1022; Physiology
Lecture Content[]

{kind=link}
Electrical conduction is proliferated by cardiac myocytes connected by gap junctions. Desmosomes lie between these gap junctions. It takes about .22 seconds for full conduction. There is slow conduction through the AV node due to it being surrounded by fibrous tissue. Excitation originates in the sinoatrial node, there is internodal pathways in the atria (conduction velocity 0.03m/s), atrioventricular node (slowed, 0.05m/s), bundle of His, Purkinje fibres (3-5m/s, rapid). Conduction spreads through the atria in about 0.09 seconds and through the ventricles in about 0.06 seconds.
AV node is surrounded by annulus fibrosis, slow conduction is to allow flow from atria to ventricles. Arranged from the base upwards so that maximum blood is squeezed out of the ventricles
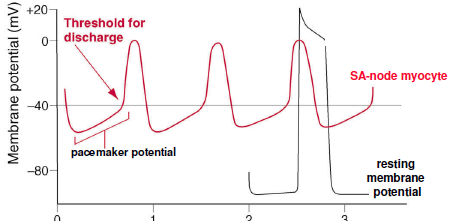
Pacemaker potential has no stable resting potential, has less negative maximum diastolic potential. Ventricular action potential has stable resting action potential, plateau phase. Plateau phase is slow to prevent tetany
{kind=link}
Membrane potential is determined by differences between extracellular and intracellular ions. There is more Na outside the cells (145mM), 15mM inside cells, increased Ca outside the cells, and increased K inside the cells. The potential in the cardiac myocytes is -80mV. Depolarisation is by fast Na channels then slow Ca channels. Ca influx contributes to plateau by maintaining potential. Repolarisation is by outward K channels.

{kind=link}
SA node is the pacemaker. There is no fast sodium influx.
ECG measures excitation of the heart, some parts are positively and some negatively charged. Small currents can be detected at the body surface. It is used to determine the shape and relative size of the chambers, disturbances in rhythm and conduction, the extent and damage of damage to the myocardium, and the effects of drugs and abnormal concentration of various plasma electrolytes to the heart. Lead 1 views is 0 degrees, right arm -ve to left arm +ve. Lead 2 is 60 degrees, right arm -ve to left leg +ve, lead 3 is 120, left arm -ve to left leg +ve.
Normal ECG is P wave (atrial activation/depolarisation), QRS complex (activation of the ventricles) and T wave (recovery of ventricles). PR interval is time taken for depolarisation from SA to AV and His-Purkinje system to ventricles. ST segment is when entire ventricular myocardium is depolarised.
Major causes of arrythmias are shift of pacemaker to other pacemaking regions, abnormal impulse formation in the primary pacemaker, blocking or delay of conduction of impulse through the heart, spontaneous generation of abnormal impulses in any region of the heart. SA node is the pacemaker, that is why it is the sinus rhythm. Conditions that block the impulse through the AV node are ischaemia, compression of the AV node by scar tissue, inflammation of the AV node (fever), extreme stimulation of the heart by the vagus nerves (rare).
Sympathetic nerve activation is the accelerator. Increase rate of generation of pacemaker action potentials thus HR. Happens up to 230bpm. Parasympathetic is the brakes, decreases rate of generation of pacemaker action potentials, can decrease heart rate down to 20bpm. Autonomic nerve stimulation blocks para/symp activity, heart rate is 100bpm. Heart is normally under vagal tone. Adrenaline increases heart rate.
Exercise rate reduces resting heart rate. Maximum heart rate decreases with age. Maximum heart rate is about 220-age. Heart rate is inversely proportional to body size.