Lecture Details[]
Robert Widdop; Week 11 MED1022; Pharmacology
Lecture Content[]
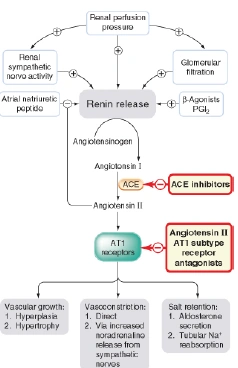
CHF has decreased heart output, CO cannot meet metabolic demands. Caused by coronary disease/atheroschlerosis, AMI, ischaemia, angina, arrhythmias, hypertension, cardiomyopathy, cardiac valvular disease. Preload is stretch, increased by increased blood volume, venoconstriction. Afterload is increased by arterial/peripheral vasoconstriction. Increased preload increases CO, increased afterload decreases CO. Acute symptoms are tachycardia, SOB, oedema, decreased exercise tolerance. Chronic symptoms are arrhythmias, hypertension, oedema, cardiomegaly. NYHA level I- no symptom limitation with ordinary physical activity, II is normal PA somewhat limited by dyspnoea, III is exercise limited by dyspnoea with moderate workload, IV is dyspnoea at rest or with little exertion. Decreased CO increases SNS. Decreased renal perfusion increases RAS (ang II, aldosterone).
{kind=link}
Treatment of CHF can be due to lifestyle changes; decreased cardiac workload (diuretics, vasodilators such as beta blockers, RAS inhibition), increased cardiac contractility from positive inotropes such as digoxin and dobutamine. Diuretics such as thiazide work on distal tubule (hydrochlorothiazide), loop diuretics act on loop of Henle (frusemide), potassium sparing diuretics act on collecting tubules and ducts (spitonolactone). Digoxin toxicity can be increased unless potassium sparing diuretics are used. Thiazide and loop side effects include rash, hypokalaemia, hyperuricaemia, glucose intolerance, hypercholesterolaemia. Hypovolaemia, hearing loss and increased Mg/Ca excretion is more common in loops. Hypokalaemia can cause arrhythmias, increased digoxin toxicity, neuromuscular weakness and constipation, drowsiness, irritability, confusion. There are two classes of K sparing diuretics- aldosterone antagonists (spironolactone) and sodium channel blockers (amiloride) which act at distal tubule/collecting duct. Eplerenone is second generation aldosterone antagonist. ACE inhibitors and AT1 receptor antagonists can also be used. Nitrovasodilators and hydralazine are other vasodilators, may be used when ACE/AT1R are contraindicated or not well tolerated.
Beta adrenoreceptor antagonists can be non-selective (propanolol) or cardioselective (atenolol). Side effects include cold extremeties, provocation of asthma, heart failure, diabetes. It decreases the sympathetic drive to heart from NA, removes critical symp compensation of failing heart. Beta blockers are added to conventional therapy when the patient is stable, increasing dose slowly. Treatment is with lifestyle changes, decreased cardiac workload (diuretics, vasodilators), increased cardiac contractility with positive inotropes (digoxin, dobutamine). Digoxin inhibits Na/K ATPase and increases myocardial intracellular calcium. Leads to increased contractility and reduced oxygen use in failing heart. Causes increased cardiac output, is more effective in cardiomyopathies and less in CHF secondary to hypertension. Digoxin can cause vagal stimulation which causes bradycardia, increased PR interval, reduced AV contraction (can be used in flutter). High doses cause membrane depolarisation with increased abnormal automaticity, various ventricular arrhythmias. It has a narrow safety margin, absorption is 75% so minor changes in levels may cause toxicity, it has a long half life of 30-40hrs, may need loading dose. Digoxin is mainly excreted in kidneys, reduced clearance in renal disease, antibodies for overdose. Can cause arrhythmia, anorexia, vomiting, nausea, vagal stimulation, visual disturbances, agitation, hallucination. Fall in potassium or increase in calcium can cause toxicity. Positive inotropes such as b1 adrenoreceptor agonists have limited IV use due to b1 adrenoreceptor downregulation in CHF.
Step care: Na and weight restriction diet; diuretic or ACE inhibitor; combine classes; add 3rd eg digoxin; add 4th eg b blocker, spironolactone, epleronone.