Lecture Details[]
Norm Eizenberg; Week 3 MED1011; Anatomy
Lecture Content[]
Articular system is the system of joints in the body. They can be fibrous for no movement, cartilaginous to withstand pressure, or synovial for movement.
Fibrous joints can be suture joints (seam), syndesmosis (bind together bones), or gomphosis (in teeth and nails).
Primary cartilaginous joints are bones linked by hyaline cartilage (eg epiphyseal plate). Their binds are very strong. Periosteum is continuous with perichondrium.
Secondary cartilaginous joints are fibrocartilage with hyaline cartilage on each side eg IV disc. They are located in the midline only.
Synovial joints are a synovial cavity filled with synovial fluid enclosed in a fibrous capsule. They can be simple, with one pair of articular surfaces, compound with more than one pair of articular surfaces, or complex when they are partitioned into more than one cavity. Types of synovial joints are plane (spine facet joints), hinge (elbow, 1 axis), condylar (2 axes, MP joints), ball and socket (3 axes, shoulder).
Articular surfces are typically bony surfaces occasionally surrounding non-articular areas. They are smooth and reciprocally curved, and may not be bony (eg disc, meniscus, ligament). They are covered by hyaline articular cartilage. Hyaline cartilage is weightbearing, avascular and aneural, and frictionless. It protects the otherwise exposed nerves and vessels that supply the bony articular surfaces, and recieves nutrition from synovial fluid and the bone underlying the articular cartilage.
Joint degeneration is caused by thinning and loss of articular cartilage, can cause articulation of bony surfaces without cartilaginous protection, exposes raw nerve endings from the bone which can cause severe pain.
Osteophytes can form and enroach on foramina causing pain. Injury to articular cartilage, commonly from fracture, can cause damage to the hyaline cartilage. If a fragment of cartilage breaks off, a loose body is created with an associated defect that may expose underlying bone. Damage to articular cartilage triggers early onset degereative arthritis. A loose body can survive or grow in synovial capsule, may produce intermittent locking of a joint if caught.
Fibrous capsule encloses a joint defining its boundary. Attaches to articular margin (except where it doesn't). Reinforced by ligaments and sometimes by tendinous insertions of adjacent muscles. Has a rich nerve supply for pain and proprioception. It is initially attached to the epiphysis and can migrate either way, usually toward articular surface.
Synovial membrane is a serous membrane that lines all non-articular surfaces on the joint interior. It has a rich blood supply and secretes synovial fluid into the joint cavity (1cm3). Synovial fluid is nutrient to articular cartilages, contains hyaluronic acid and its viscocity varies inversely to shear stress. Synovial effusion is an accumulation of synovial fluid, usually caused by irritation of the synovial membrane by mild, repeated trauma causing dilation of vessels and a subsequent increase in secretion of synovial fluid. It produces swelling of the joint. Tissue resistance limits degree of effusion.
Haemarthrosis is an accumulation of blood in synovial cavity, typically due to severe trauma but can be with minimal trauma in haemophiliac. Tissue resistance limits expansion of blood accumulation. Produces a swelling both painful and warm to touch.
Septic arthritis is an accumulaiton of pus in the joint cavity, can be from direct introduction of microbes into synovial cavity or indirect from bloodstream spread of infection. May lead to permanent damage from erosion of articular cartilage/surfaces.
Ligaments are fibrous links between periosteum of one bone to another. May be thickenings of capsule or separate from it, and resists distraction of articular surfaces. They have poor blood supply and rich nerve supply, and is vulnerable to injury if in discrete parts. An intracapsular ligament is oriented along the axis of movement. Its strength is proportional to stresses carried. Collateral ligaments are medial and lateral, prevent unwanted movements. White ligaments are collagen, resist stretching and remain elongated once stretched. They are found in joints where movements are limited. Yellow ligaments are elastin, allow stretch but return to original position after use.
Ligament injuries (sprains) are common, particularly in adults, and are caused by damage to collagen fibres. Microscopic sprain is grade I; partial tear is grade II; and complete tear is grade III. Ligaments tear at their weakest point, which is generally their insertion into bone. (at or near their attachments). Sometimes bone can be avulsed with the ligament.
Abnormal joint movement is associated with ligament tears but this may be masked by muscles (reflex spasm). Stressing a ligament to elicit pain is also diagnostic, in grade III tears sensory fibres are likely severed so may not elicit response. Laxity of a ligament from injury may predispose to future injury. Loss of proprioception also does this.
Special structures: articular- labrum, disc/menisci; extrasynovial- intracapsular tendon, fat pad; extracapsular-
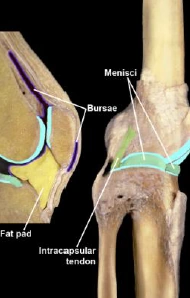
{kind=link}
bursae
Labrum is fibrocartilaginous, deepens a ball and socket joint. A disc (menisci) enables separate set of joint movements to occur either side, increases articular surface to reduce stress at any one point, shock absorber, assists in spread of synovial fluid. A torn labrum tends not to heal as it is avascular. Tears to disc and menisci also tend not to heal except at periphery, where they recieve a blood supply. A meniscus trapped between bony condyles may split longitudinally. A dislodged fragment of meniscus may survive as a loose body in a joint cavity.
Bursae tend to be more numerous at joints with greater mobility. Excess secretion of synovial fluid into a joint may also be transferred to communicating bursae. Bursitis can occur from unaccustomed or repetitive movement; can collect synovial fluid, blood or pus. Infection in a bursa can spread to synovial cavity. A fat pad can become pinched between bony surfaces, can cause pain associated with bony effusion.
Stability is inversely related to mobility. Close packed position is that of most stability, articular surfaces are locked and ligaments are maximally taut, also the position of least volume in synovial cavity (and most pain if infection is present).
Joint separation is most likely when overlying muscles are relaxed or weakened, stretching or tearing of capsule and ligaments, reflex muscle spasm tends to protect from further damage, may be subsequent ligamentous laxity.
Articular vessels form a vascular circle at the capsular attachment to supply capsule as well as bone, many vascular foramina are for veins. Anastomosis with major vessels tends to occur around a joint.